As an Amazon Associate I earn from qualifying purchases.
Sciatica Explained: Causes, Symptoms, and What Actually Relieves Nerve Pain
A clear, evidence-based guide to sciatica that explains what it is, why it happens, what truly helps relieve nerve pain—and how to avoid common mistakes that can make symptoms worse.
2/9/20267 min read


Sciatica: What It Is, Why It Happens, and How to Treat It Without Making It Worse
Sciatica has a special talent for turning ordinary life into a dramatic production. One day you’re bending to pick up laundry; the next, your leg is sending sharp, electric complaints down to your calf that almost knock you off your feet. People often describe it as “back pain,” but sciatica is more specific than that and understanding that difference can save you weeks of frustration. Here’s the part most people don’t hear early enough: many common “back pain” fixes can accidentally irritate sciatica, while the strategies that help most can feel almost too simple to be true. The real question is whether your symptoms are coming from a briefly annoyed nerve that needs calming or a nerve that’s being repeatedly provoked by the same few patterns every day. If you can spot which one you’re dealing with, the path forward gets a lot clearer.
Sciatica isn’t a disease by itself. It’s a symptom...
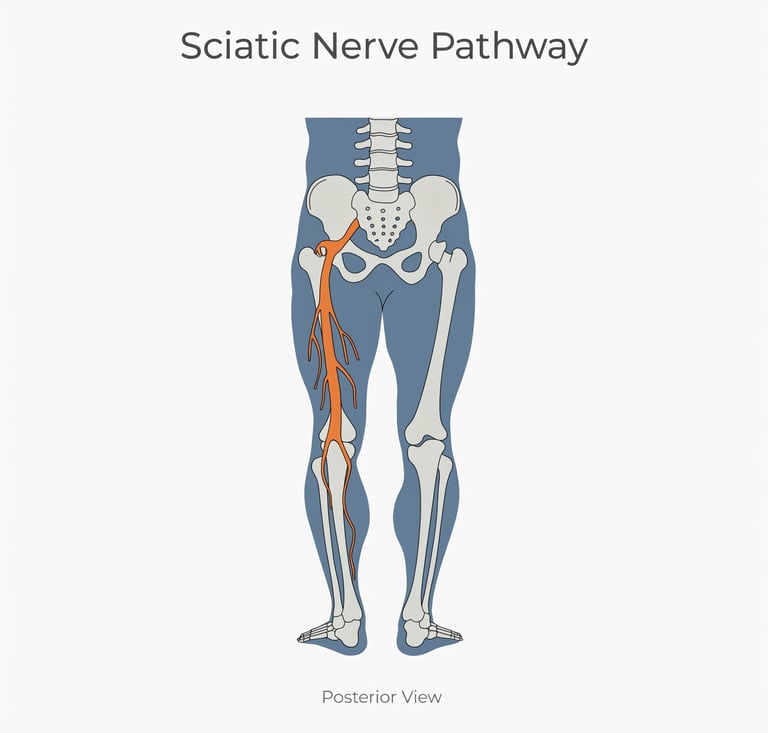
Sciatica isn’t a disease by itself. It’s a symptom—a signal that the sciatic nerve (the body’s largest nerve) is irritated or compressed. MedlinePlus, a National Library of Medicine resource, describes sciatica as pain, weakness, numbness, or tingling in the leg caused by pressure on or injury to the sciatic nerve. That nerve begins in the lower back, travels through the buttock, and runs down the back of the leg, supplying sensation and helping control muscles in the lower limb. When the nerve is angry, symptoms can radiate—often on one side—down the thigh, into the calf, foot, or toes.
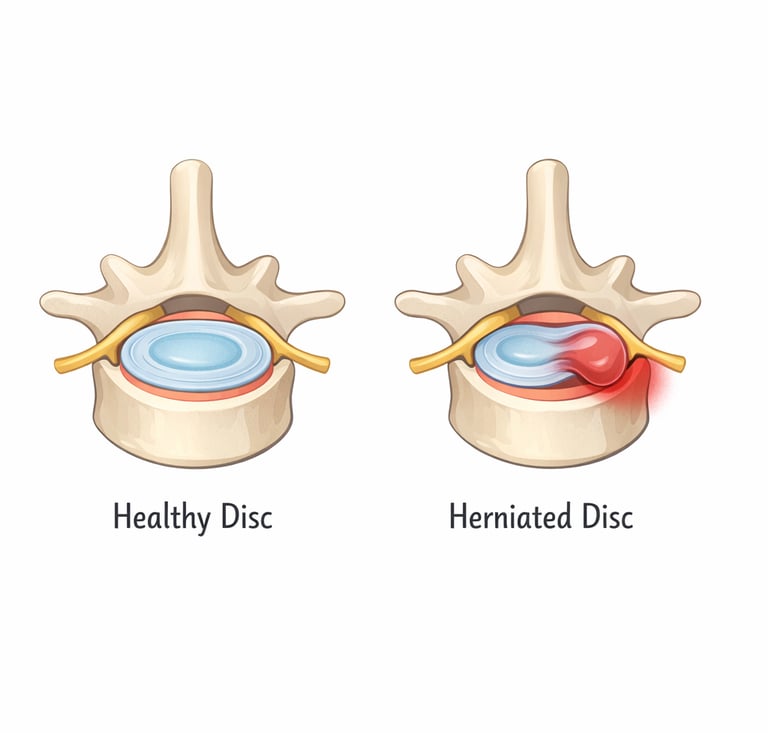
So how does the nerve get irritated in the first place? The most common culprit is a herniated (or “slipped”) disc, where the cushioning disc between spinal bones bulges or leaks and presses on a nearby nerve root. Spinal stenosis (narrowing of spaces in the spine), spondylolisthesis (one vertebra slipping relative to another), and some less common issues—like piriformis syndrome or tumors—can also be responsible. What matters for treatment is not only what caused it, but how your symptoms behave: do they flare with sitting, bending, coughing, or sneezing? Do they ease when you walk? Do they “travel” down the leg or start to retreat back toward the hip? Those patterns tell clinicians more than most people realize.
A key point that surprises many readers is that sciatica can feel terrifying while still being highly treatable. Many cases improve over time, especially when you stop feeding the irritation cycle. Major trials comparing early surgery with conservative care show that people often improve in both groups; surgery tends to relieve leg pain faster for severe, persistent cases, but longer-term outcomes can be similar. In a well-known randomized trial in The New England Journal of Medicine, early surgery produced faster pain relief and perceived recovery, yet by one year the overall likelihood of recovery was very high in both the early-surgery and conservative-care groups. A follow-up randomized trial report in BMJ echoed the same theme: faster relief with early surgery, but similar outcomes by one year, with some people still reporting unsatisfactory results at two years—an important reminder that surgery is a tool, not a magic wand.
Because sciatica can be intense, people often rush to imaging. That’s understandable—pain makes us want certainty—but it’s not always helpful early on. The UK’s National Institute for Health and Care Excellence (NICE) advises that people with low back pain with or without sciatica should not routinely have imaging requested by non-specialist services unless serious underlying pathology is suspected, because imaging findings are common and often unrelated to symptoms and can cause unnecessary distress. (NICE) In other words: an MRI can show disc changes that sound scary on paper, even when those changes aren’t the true reason you hurt—or aren’t something that requires aggressive intervention right away.
So what does good treatment look like when you’re not trying to “outsmart” your nervous system with panic? Most credible medical sources land on a similar starting point: keep moving in ways that don’t spike symptoms, avoid prolonged inactivity, and use symptom-guided care. Mayo Clinic notes that while resting for a day may help, staying inactive can make sciatica worse, and it recommends practical home approaches like alternating cold and heat and gentle stretching (held long enough to be meaningful). MedlinePlus similarly emphasizes that many cases recover with conservative treatment and includes common first-line measures like heat/ice and appropriate pain relief strategies, along with evaluating the underlying cause.
One of the biggest “what not to do” items is also one of the most tempting: extended bed rest. People feel better lying down, so they conclude lying down is the treatment. Research suggests it’s not that simple. Cochrane, an international nonprofit known for rigorously reviewing medical evidence, summarized randomized trials and found that for acute low back pain, advice to stay active can offer small improvements compared with bed rest; for sciatica specifically, results showed little or no difference between bed rest and staying active, and prolonged rest can carry downsides like deconditioning. The practical takeaway for sciatica isn’t “go run a 10K.” It’s “don’t turn your life into a mattress audition for weeks.” Short rest may be reasonable when symptoms are very pronounced, but your goal is a return to tolerable movement as soon as you can.


Another common mistake is stretching or “mobilizing” straight into nerve pain because you’ve been told tight muscles are the problem. Sciatica often behaves like an irritated electrical cable: yanking harder doesn’t soothe it, it shocks you. When stretching increases sharp, shooting, burning, or tingling sensations down the leg, that’s a sign the nerve is being aggravated, not “opened up.” A better approach is movement, like sciatic nerve flossing, that calms symptoms over the next several hours and especially the next day. Clinicians often watch for whether symptoms “centralize,” meaning the pain retreats out of the leg and becomes more local—less leg, more buttock or back. That pattern can be a good sign that the nerve is less provoked.
Physical therapy can be especially useful here, not because it’s magic, but because it helps you find the movements your symptoms tolerate and then build your capacity around them. The best therapy for sciatica typically looks less like random stretching and more like a progressive plan: graded walking, strength work that doesn’t flare symptoms, and positions that reduce nerve sensitivity. NICE recommends exercise as a core part of managing low back pain and sciatica, and it also notes that manual therapy (like mobilization or soft tissue work) should be considered only as part of a broader treatment package that includes exercise (and sometimes psychological approaches when fear or avoidance becomes a barrier to recovery). That last part matters: sciatica can make people afraid to move, and fear-driven avoidance can quietly prolong disability. A plan that rebuilds confidence is often as important as the plan that strengthens muscles.
When pain is severe enough to block movement, medical options can be reasonable bridges. Epidural steroid injections are often discussed for sciatica caused by lumbar disc herniation, and the evidence suggests they can help some people, mainly in the short to medium term. A 2024 systematic review and meta-analysis of randomized trials found epidural steroid injections provided short- and medium-term pain relief for sciatica from lumbar disc herniation, while long-term effects were limited and improvements in nerve function were not clearly significant. That lines up with the way many pain specialists frame injections: not as a cure, but as a window of relief that can make rehab and daily activity possible again.




Now for a few “what not to do” moves that are less talked about, but very common. One is treating sciatica like a purely structural problem that must be “put back in place” immediately. Sometimes the body needs decompression; sometimes it needs strength; sometimes it needs time for inflammation around a nerve root to calm down. But chasing aggressive adjustments, intense stretching, or repeated treatments that flare symptoms can create a cycle where the nerve never gets to settle. Another is ignoring the basics that make nerves more irritable: poor sleep, high stress, and long periods of static posture. Your sciatic nerve doesn’t live in a vacuum, it lives in a human being with a nervous system that responds to load, threat, and recovery.
Because this is a Bounce Back–style guide, it’s also important to say plainly: there are moments when “wait and see” is not the vibe. If you develop progressive weakness, significant numbness in the groin/saddle area, or bowel/bladder changes, that’s not a “stretch it out” situation. That’s a “get evaluated urgently” situation. Even in everyday cases, persistent sciatica that is worsening, not improving over weeks, or severely limiting function deserves a clinician’s eye, especially to rule out less common causes and to consider whether additional interventions (like injections or surgery) would meaningfully change your trajectory.


So where does that leave you if you’re reading this because your leg feels like it’s buzzing, burning, or threatening to file a complaint with HR? It leaves you with a surprisingly grounded strategy: treat sciatica like an irritated nerve that needs both respect and reconditioning. Respect means avoiding what spikes symptoms and limiting prolonged inactivity. Reconditioning means gradually reintroducing movement and strength in ways your symptoms tolerate, and using medical options as bridges when pain blocks progress. The evidence from trusted medical references and large clinical trials supports the idea that many people recover—often without surgery—and that choosing the right level of intervention at the right time is what changes the experience from “I’m stuck” to “I’m improving.”
If you want help sorting out your specific pattern—what flares you, what calms you, and what your “next right step” should be—this is exactly what the Bounce Back community is for. Bring your questions, your weird symptoms, your wins, your setbacks, and your “is this normal?” moments. You don’t need to become a spine expert to get your life back—you just need a plan, some support, and the confidence to move forward.